
For many people who wish to improve health and body composition, the primary objectives typically involve consuming more vegetables, fruits, and protein, limiting high-calorie food choices, and exercising regularly. In many cases, taking these steps can often produce excellent results.
At some point, however, fat loss no longer becomes so simple. For individuals who are already moderately lean, but hoping to achieve additional fat loss, the body will begin to thwart these efforts through adaptive responses designed to prevent starvation. Although these responses were undoubtedly useful for our ancient ancestors, they have become maladaptive in an environment in which calories are infinitely plentiful.
Once athletes reach a certain level of leanness, one of the primary objectives of their fat loss plan will likely need to revolve around circumventing what is frequently referred to as “starvation mode”.
What exactly is “starvation mode”?
When the body becomes threatened with the risk of starvation, the following physiological responses occur:
- Decreased leptin, increased ghrelin, increased hunger (1-8)
Increased hunger is the hallmark trait of starvation mode, and the primary mechanism through which the body attempts to halt fat loss. The longer you spend in starvation mode, the more that hunger will become increasingly unbearable, eventually forcing you to eat more.
- Diverted cognitive attention towards food cues, decreased intelligence (9-17)
When people are in a caloric deficit, the brain begins reserving a section of working memory specifically for seeking out and responding to any signs of food in the area.
According to an fMRI study conducted by Stice, Burger, & Yokam (9):
“Youth in a longer-term negative energy balance likewise showed greater activation in attention (anterior cingulate cortex, ventral medial prefrontal cortex), visual processing (superior visual cortex), reward (caudate) and memory (hippocampus) regions in response to receipt and anticipated receipt of palatable food relative to those in neutral or positive energy balance.”
As a result, when lean people are on a diet, their thoughts tend to become be preoccupied by thoughts of food.
Interestingly, because a significant amount of cognitive resources are being diverted towards seeking food, this has been repeatedly demonstrated to result in an overall decrease in intelligence and cognitive capacities while actively in the process of dieting.
- Decreased thyroid hormones (18-24)
Decreased thyroid hormones can lower metabolism and also lower body temperature (25), potentially leading to reduced energy levels and eventually an impaired capacity for further weight loss.
Additionally, decreased thyroid hormones may also lead to decreased blood flow to the adipose tissue (26), making the fat stored in the belly region even more resistant to fat loss than it normally is.
- Decreased testosterone and estrogen (26-30), altered cortisol functioning and stress reactivity (31-34)
These hormonal changes can lead to extreme decreases in energy and can unfavorably affect overall body composition.
- Decreased Non-Exercise Activity Thermogenesis (NEAT) (35-47)
When people are deprived of calories, their body starts becoming more “energy efficient” and expends less energy during everyday tasks of life. Small motions, such as fidgeting, become inhibited, and overall metabolism decreases, making it harder to lose weight.
Interestingly, individuals appear to exhibit highly variable responses in regards to changes in NEAT. Some people display a “thrifty phenotype” and decrease their metabolism by hundreds of calories per day, some people barely decrease their metabolism at all, and a very rare percentage of people somehow seem to increase their NEAT in the presence of calorie restriction.
It appears that this feature of metabolism is highly genetic, and the people who exhibit the highest decrease in NEAT are those who come from populations that were historically subjected to extreme famine, such as the Samoans or Pima Indians (48-57).
Summarizing Starvation Mode
The body exhibits multiple hormonal, cognitive, and metabolic responses to calorie deprivation that can make it difficult for advanced athletes to achieve their desired level of leanness. These adaptations cause us to eat more, burn less calories per day, and feel overall sluggish and miserable during times of calorie restriction.
Starvation Mode is Not Permanent
Fortunately, none of the consequences of starvation mode are permanent. When normal eating is resumed, leptin, ghrelin, thyroid hormones, and sex hormones will return to normal (58-60). This typically occurs within a couple of weeks of returning to caloric equilibrium (58-59). In extreme cases, however, such as preparation for a bodybuilding contest, studies have found that subjects may require months of eating at caloric equilibrium before hormones fully normalize (60).
How do I know if I’m experiencing signs of starvation mode?
The number one sign of starvation mode is extreme hunger. If you are not experiencing major hunger issues, then you are definitely not undergoing any starvation responses. If your diet is very high in satiating foods such as vegetables, fruits, protein, and water, and you are still struggling to combat hunger, this could be your body’s starvation responses fighting back.
Along with increased hunger, another major indicator of starvation responses is a decrease in body temperature due to lowered thyroid hormone and overall metabolism (25). To check this, you can use a thermometer to establish a “baseline” temperature by measuring every day for a couple of weeks while you are not actively trying to lose fat. Then, continue tracking as you begin your fat loss plan and look for any continuous dips in body temperature that might indicate your body is beginning to adapt.
“Starvation Mode” Becomes Increasingly Relevant for Leaner Individuals
Starvation mode is less likely to become apparent in individuals with a higher body fat percentage, and becomes increasingly more likely as body fat percentage decreases.
Thankfully, multiple techniques can be employed to combat this issue.
The first strategy that can be used for avoiding starvation mode is:
#1: Eat More (A Lot More) and Develop Elite Levels of Endurance
Multiple studies have found that very low calorie diets – as low as 800 calories/day – can be safe and effective for overweight individuals (61-62). For advanced fat loss clients, however, this approach is a disaster.
Let’s imagine two hypothetical individuals:
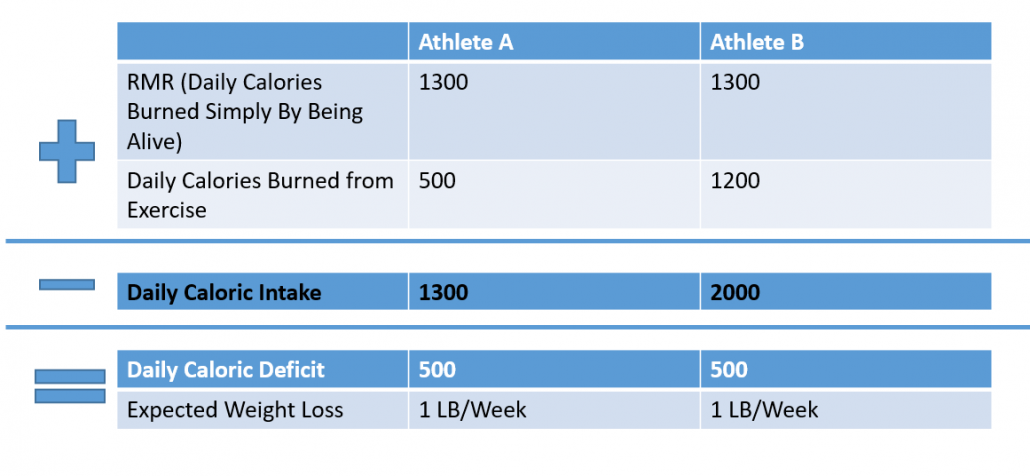
If you add up the RMR and the calories burned through exercises, then subtract the calories consumed, both athletes are creating a deficit of approximately 500 calories/day, which should theoretically yield 1 pound of fat loss per week.
In theory, since the calorie deficits are the same, both people should enjoy relatively equivalent amounts of fat loss, right?
Actually, this could not be further from the truth, and is one of the biggest misconceptions that many advanced fat loss clients are mislead by.
Low Caloric Intake, Rather than Fat Loss, is the Primary Trigger of Starvation Mode
Many people believe that “starvation mode” is an automatic response to any sign of weight loss when body fat stores are already low. The reality, however, appears to be that starvation mode is more directly triggered when low body fat stores are coupled with low caloric intake. Amazingly, weight loss in the presence of high caloric intake does not create as pronounced of a starvation response.
In the example above, Athlete B, who is eating more but also exercising much more, will not suffer the same starvation responses that Athlete A will experience. She will experience less hunger, less fatigue, less of a drop in metabolism, and will not only end up losing more fat, but will also be much less likely to ultimately regain the weight once she returns to normal eating.
Therefore, high-calorie diets can be extremely powerful for circumventing starvation mode and promoting fat loss in advanced clients.
Examining the Research
Let’s take a look at the research literature for a more detailed look on how important this strategy can be:
In a study by Alajmi et al (63), 12 subjects were required to either reduce their daily calorie intake by 837 calories or to perform 837 calories worth of exercise. When food intake was reduced, blood tests revealed heightened concentrations of plasma acylated ghrelin. Appetite increased dramatically, and the subjects consumed significantly more calories when later given the opportunity to eat.
When an equivalent calorie deficit was created via exercise, however, none of these adaptations were present. Ghrelin levels did not increase above baseline, appetite did not increase, and the subjects did not consume more food when given the chance to eat.
In a study by Cameron et al (64), 10 subjects were required to either reduce their daily calorie intake by 25% or to perform an equivalent amount of exercise. In the diet group, appetite increased significantly, and subjects consumed more calories when later provided with the opportunity to eat. The exercise group, however, did not display altered appetite or food consumption compared to baseline.
In experiments by Foright (65), 11 overweight subjects were instructed to either reduce their calorie intake or increase their physical activity. After months of following this protocol, both groups of subjects lost approximately the same amount of weight. The diet group, however, reported significant increases in hunger and a small decrease in metabolism. The exercise group, however, exhibited no change in hunger, no change in metabolism, and no symptoms of starvation mode.
In an observational study by Hume (66), 229 subjects were analyzed for resting metabolic rate, body fat percentage, and daily calorie intake using doubly-labeled water assessments (which tend to be highly accurate). These subjects were then tracked over the course of multiple years.
At the beginning of the study, the average body fat percentage of the subjects was around 18.5% body fat. After three years, the subjects who were following a high-calorie diet coupled with low exercise increased their body fat percentage to an average of 22.3%. Surprisingly, however, the subjects who were following a low-calorie diet combined with a low amount of exercise still ended up increasing their body fat percentage to an average of 21%.
On the other hand, the subjects who consumed a high-calorie diet combined with a high amount of exercise actually decreased their body fat percentage to an average of 15.9%.
All of these studies appear to be pointing to the same conclusion: people consuming a low-calorie diet will experience significantly more pronounced starvation responses compared to individuals in an equivalent calorie deficit who are consuming a higher calorie diet.
Abs are Made in the Gym, Not the Kitchen
Proper nutrition is essential for achieving optimal health and fitness. At some point, however, you can only cut your calories so low. Once you hit a weight loss plateau, there eventually comes a point at which you can’t simply keep cutting calories lower.
The leaner you become, the less you can rely on dietary modifications for continuing to make progress and the more and more you need to start emphasizing changes to your exercise routine. Creating a caloric deficit through large volumes of exercise, rather than very low-calorie diets, is the best strategy for continuing to lose fat without suffering the consequences of the body’s starvation defenses.
Which Exercise is Best?
When it comes to exercise, most experts advocate that strength training, rather than the cardio, is the superior form of exercise for fat loss. Many studies have found that weight-lifting is more important than cardio for losing body fat (67-76).
I do not disagree with the findings of these studies – I do believe that strength training is extremely important for fat loss – but I also believe that at some point, increased volume of strength training leads to diminishing returns.
Most of the aforementioned studies involved subjects who were performing only a few hours of exercise per week. For advanced fat loss clients who are exercising more than 7 hours per week, I believe that the bulk of this time should be spent towards endurance training, which burns significantly more calories than strength training.
Improved Endurance = Higher Calorie Burn
As endurance improves, a greater distance can be covered in less amount of time, resulting in an increased amount of calories burned per hour.
In addition to eating more calories, there is another strategy that I recommend in order to ensure that starvation responses do not thwart fat loss efforts:
Strategy #2: Alternate Distinct Phases of “Cutting” with Distinct “Maintenance” Periods to Allow Your Body to Reset
At any given time, there are three situations that your body can be in:
- Caloric Equilibrium (aka “Maintenance”): The amount of calories you are consuming is approximately equal to the amount of calories you are burning
- Caloric Deficit (aka “Cutting”): The amount of calories you are consuming is less than the amount of calories you are burning
- Caloric Surplus: The amount of calories you are consuming is greater than the amount of calories you are burning
When you spend a prolonged period of time in a caloric deficit, and are consistently lifting weights and consuming protein, your body fat percentage will eventually decrease.
Unfortunately, however, the longer you spend in a caloric deficit, the more susceptible you become to the risks of starvation mode, which means that steps must be taken in order to reset the body back to normal.
The Truth About “Cheat Meals”
One strategy that is commonly employed to prevent starvation mode and “reset metabolism” is the use of “cheat meals” or “cheat days”. Unfortunately, from a physiological perspective, one cheat meal or cheat day is not enough.
According to research, you need to spend a over a week in a caloric equilibrium “Maintenance” phase before hormones will return to normal (58-59) – one cheat meal or cheat day simply won’t cut it.
This is nicely summarized by author Lyle Mcdonald:
“…thyroid hormones and the effects that they exert aren’t immediate. It may take 7 days of eating at maintenance for thyroid levels to come back to normal, but you need at least another week to get many of their effects to max out. So in answer to the question “Can I make the break shorter?”, the answer is “No.”
Rather than simply eating “cheat meals”, a more effective approach towards preventing starvation mode is to take a long break from Cutting in order to provide the body with a sufficient opportunity to reset.
Examining the Research Literature
Let’s take a look at the research literature for some examples of how valuable this strategy can be:
In a study by Byrne et al (77), 36 subjects were assigned to either a continuous, calorie restricted diet for 16 weeks or an “intermittent” diet that involved alternating between two weeks of Cutting and two weeks of Maintenance. The subjects who alternated between phases of caloric deficit and caloric equilibrium ended up losing significantly more fat than the continuous dieters.
In experiments by Davoodi et al (78-89), subjects were instructed to follow a traditional calorie-restricted diet for six weeks, or follow a special diet alternating between 11 days of calorie restriction and 3 days of normal eating. The subjects who alternated between 11 days of “Cutting” followed by 3 days of “Maintenance” ended up losing significantly more fat and felt significantly less hungry.
Interestingly, this effect is not confined to humans. Seimon et al (80) conducted a similar experiment on mice. Mice that alternated between 5-6 days of calorie restricted eating followed by 1-3 days of normal eating lost significantly more fat than mice who had their caloric intake continuously restricted for 22 weeks.
All of these studies essentially came to the same conclusion: the subjects who spent less time in a caloric deficit actually ended up losing more fat.
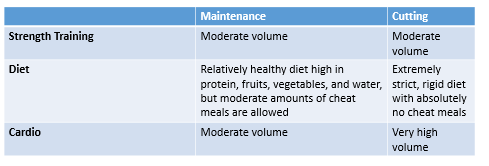
Defining Cutting and Maintenance
Cutting and Maintenance phases should differ as follows:
The goal is to alternate between each phase: approximately two weeks of hard Cutting to quickly drop fat, and two weeks of Maintenance to allow the body to “reset” and become comfortable at the new weight.
It doesn’t have to be an exact 2 weeks:2 weeks ratio. For example, you could do one week of Cutting followed by 2 weeks of Maintenance or 2 weeks of cutting followed by 3 weeks of Maintenance if you are willing to be more patient. The only rule is that you must never allow the Maintenance phase to last less than 2 weeks.
Following this approach, the goal for most people should be to lose approximately 1 lb per week during the Cutting phase, and then to maintain this new weight for two weeks during the Maintenance phase. For smaller individuals (less than 130 lb), you may only be able to drop 0.5 pounds per week during the Cutting phase.
The Pitfalls of Maintenance Phases
Although this approach is reasonably simple, my experience is that many of my clients have a very difficult time alternating between “Cutting” and “Maintenance”, and as a result, many of them become unsuccessful with reaching their final fat loss goals.
The reason that many individuals struggle is that they have a hard time staying adherent to the plan during the Cutting phase, yet ironically, they push themselves too hard during the Maintenance phase. Instead of separate, distinct phases, they end up in some perpetual “hybrid” half-Maintenance half-Cut diet/exercise regimen that seems to last for months but never seems to make them feel that they are moving closer to their goals.
During the Cutting phase, it is essential not to skip workouts and to keep the volume of cardio high. Additionally, during this time, adherence to the dietary plan needs to be close to perfect.
Conversely, during the Maintenance phase, it is important to cut back on the overall volume of cardio and consume multiple cheat meals throughout the week. Don’t binge, but don’t restrict yourself completely – find the right balance of moderation.
When it comes to cheat meals, carbohydrates appear to be vastly superior compared to fats or protein for resetting leptin levels (81-82) that may have plummeted due to the body’s starvation responses. For this reason, I do not recommend very low-carb or keto type diets during this time.
Although it may be very difficult for many people to become comfortable with the distinct separation of Cutting and Maintenance phases, this skill is invaluable for reaching and maintaining a low body fat percentage without suffering from intense hunger or weight regain.
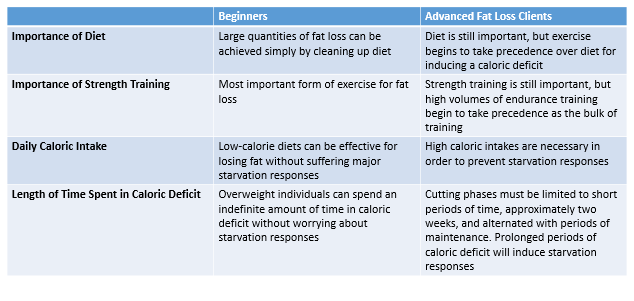
Putting it All Together
As you can see, fat loss for an advanced client is very different and much more complicated than fat loss for a beginner. While beginners can often lose large amounts of fat simply by improving their diet and lifting weights a few times per week, advanced clients may need to combine a healthy diet and resistance training plan with large amounts of cardio and strategic bouts of fat loss and maintenance phases.
As a result, a fat loss program for an advanced client may look something like this:
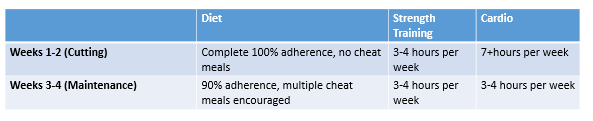
This cycle would be repeated indefinitely until the target body fat percentage has been achieved.
Pros and Cons
The disadvantage of this approach compared to the “traditional” approach that most people take — very low-calorie diets for very prolonged periods of time — is that during Cutting phases, it requires spending a much greater amount of time in the gym than most people are used to.
Although this may require more time spent in the gym than most people are used to, the major advantage of this system compared to traditional approaches is that hunger, sluggishness, and the other effects associated with “starvation mode” will not be as problematic as it would be on low-calorie, continuous diets. Furthermore, the risk of weight regain will be dramatically diminished and the results of the hard work performed during the Cutting phase can last indefinitely.
Conclusions
Reaching and maintaining a low body fat percentage is difficult and is made exponentially more challenging by the body’s innate protective mechanisms against starvation. Thankfully, multiple steps can be taken to circumvent these starvation responses and achieve a healthy body composition.
References
1 Polidori, D., Sanghvi, A., Seeley, R. J., & Hall, K. D. (2016). How strongly does appetite counter weight loss? Quantification of the feedback control of human energy intake. Obesity, 24(11), 2289-2295
2 Thomas, E. A., Bechtell, J. L., Vestal, B. E., Johnson, S. L., Bessesen, D. H., Tregellas, J. R., & Cornier, M. A. (2013). Eating-related behaviors and appetite during energy imbalance in obese-prone and obese-resistant individuals. Appetite, 65, 96-102.
3 Sumithran, P., Prendergast, L. A., Delbridge, E., Purcell, K., Shulkes, A., Kriketos, A., & Proietto, J. (2011). Long-term persistence of hormonal adaptations to weight loss. New England Journal of Medicine, 365(17), 1597-1604.
4 Keim, N. L., Stern, J. S., & Havel, P. J. (1998). Relation between circulating leptin concentrations and appetite during a prolonged, moderate energy deficit in women. The American journal of clinical nutrition, 68(4), 794-801.
5 Hulmi, J. J., Isola, V., Suonpää, M., Järvinen, N. J., Kokkonen, M., Wennerström, A., … & Häkkinen, K. (2017). The effects of intensive weight reduction on body composition and serum hormones in female fitness competitors. Frontiers in physiology, 7, 689.
6 Govic, A., Levay, E. A., Hazi, A., Penman, J., Kent, S., & Paolini, A. G. (2008). Alterations in male sexual behaviour, attractiveness and testosterone levels induced by an adult-onset calorie restriction regimen. Behavioural brain research, 190(1), 140-146.
7 Derous, D., Mitchell, S. E., Green, C. L., Chen, L., Han, J. D. J., Wang, Y., … & Douglas, A. (2016). The effects of graded levels of calorie restriction: VI. Impact of short-term graded calorie restriction on transcriptomic responses of the hypothalamic hunger and circadian signaling pathways. Aging (Albany NY), 8(4), 642.
8 Fogteloo, J., Meinders, E., Frölich, M., McCamish, M., & Pijl, H. (2003). The decline in plasma leptin in response to calorie restriction predicts the effects of adjunctive leptin treatment on body weight in humans. European journal of internal medicine, 14(7), 415-418.
9 Stice, E., Burger, K., & Yokum, S. (2013). Caloric deprivation increases responsivity of attention and reward brain regions to intake, anticipated intake, and images of palatable foods. Neuroimage, 67, 322-330.
10 Burgess, C. R., Ramesh, R. N., Sugden, A. U., Levandowski, K. M., Minnig, M. A., Fenselau, H., … & Andermann, M. L. (2016). Hunger-dependent enhancement of food cue responses in mouse postrhinal cortex and lateral amygdala. Neuron, 91(5), 1154-1169.
11 Chen, P. H. A., Chavez, R. S., & Heatherton, T. F. (2017). Structural integrity between executive control and reward regions of the brain predicts body fat percentage in chronic dieters. Cognitive neuroscience, 8(3), 162-166.
12 Vreugdenburg, L., Bryan, J., & Kemps, E. (2003). The effect of self-initiated weight-loss dieting on working memory: the role of preoccupying cognitions. Appetite, 41(3), 291-300.
13 Green, M. W., & Elliman, N. A. (2013). Are dieting-related cognitive impairments a function of iron status?. British Journal of Nutrition, 109(1), 184-192.
14 Shaw, J., & Tiggemann, M. (2004). Dieting and working memory: Preoccupying cognitions and the role of the articulatory control process. British Journal of Health Psychology, 9(2), 175-185.
15 Rogers, P. J., & Green, M. W. (1993). Dieting, dietary restraint and cognitive performance. British Journal of Clinical Psychology, 32(1), 113-116.
16 Green, M. W., Rogers, P. J., Elliman, N. A., & Gatenby, S. J. (1994). Impairment of cognitive performance associated with dieting and high levels of dietary restraint. Physiology & Behavior, 55(3), 447-452.
17 Green, M. W., & Rogers, P. J. (1998). Impairments in working memory associated with spontaneous dieting behaviour. Psychological Medicine, 28(5), 1063-1070.
18 Hulmi, J. J., Isola, V., Suonpää, M., Järvinen, N. J., Kokkonen, M., Wennerström, A., … & Häkkinen, K. (2017). The effects of intensive weight reduction on body composition and serum hormones in female fitness competitors. Frontiers in physiology, 7, 689.
19 Fontana, L., Klein, S., Holloszy, J. O., & Premachandra, B. N. (2006). Effect of long-term calorie restriction with adequate protein and micronutrients on thyroid hormones. The Journal of Clinical Endocrinology & Metabolism, 91(8), 3232-3235.
20 Wadden, T. A., Mason, G., Foster, G. D., Stunkard, A. J., & Prange, A. J. (1990). Effects of a very low calorie diet on weight, thyroid hormones and mood. International journal of obesity, 14(3), 249-258.
21 Spaulding, S. W., Chopra, I. J., Sherwin, R. S., & Lyall, S. S. (1976). Effect of caloric restriction and dietary composition on serum T3 and reverse T3 in man. The Journal of Clinical Endocrinology & Metabolism, 42(1), 197-200.
22 Weinsier, R. L., Nagy, T. R., Hunter, G. R., Darnell, B. E., Hensrud, D. D., & Weiss, H. L. (2000). Do adaptive changes in metabolic rate favor weight regain in weight-reduced individuals? An examination of the set-point theory. The American journal of clinical nutrition, 72(5), 1088-1094.
23 Loucks, A. B., & Callister, R. (1993). Induction and prevention of low-T3 syndrome in exercising women. American Journal of Physiology-Regulatory, Integrative and Comparative Physiology, 264(5), R924-R930.
24 Loucks, A. B., & Heath, E. M. (1994). Induction of low-T3 syndrome in exercising women occurs at a threshold of energy availability. American Journal of Physiology-Regulatory, Integrative and Comparative Physiology, 266(3), R817-R823.
25 Soare, A., Cangemi, R., Omodei, D., Holloszy, J. O., & Fontana, L. (2011). Long-term calorie restriction, but not endurance exercise, lowers core body temperature in humans. Aging (Albany NY), 3(4), 374.
26 WENNLUND, A., & LINDE, B. (1984). Influence of hyper-and hypothyroidism on subcutaneous adipose tissue blood flow in man. The Journal of Clinical Endocrinology & Metabolism, 59(2), 258-262.
27 Hulmi, J. J., Isola, V., Suonpää, M., Järvinen, N. J., Kokkonen, M., Wennerström, A., … & Häkkinen, K. (2017). The effects of intensive weight reduction on body composition and serum hormones in female fitness competitors. Frontiers in physiology, 7, 689.
28 Govic, A., Levay, E. A., Hazi, A., Penman, J., Kent, S., & Paolini, A. G. (2008). Alterations in male sexual behaviour, attractiveness and testosterone levels induced by an adult-onset calorie restriction regimen. Behavioural brain research, 190(1), 140-146.
29 Henning, P. C., Margolis, L. M., McClung, J. P., Young, A. J., & Pasiakos, S. M. (2014). High protein diets do not attenuate decrements in testosterone and IGF-I during energy deficit. Metabolism, 63(5), 628-632.
30 Cangemi, R., Friedmann, A. J., Holloszy, J. O., & Fontana, L. (2010). Long‐term effects of calorie restriction on serum sex‐hormone concentrations in men. Aging cell, 9(2), 236-242.
31 Pankevich, D. E., Teegarden, S. L., Hedin, A. D., Jensen, C. L., & Bale, T. L. (2010). Caloric restriction experience reprograms stress and orexigenic pathways and promotes binge eating. Journal of Neuroscience, 30(48), 16399-16407.
32 Tomiyama, A. J., Mann, T., Vinas, D., Hunger, J. M., DeJager, J., & Taylor, S. E. (2010). Low calorie dieting increases cortisol. Psychosomatic medicine, 72(4), 357.
33 Rideout, C. A., Linden, W., & Barr, S. I. (2006). High cognitive dietary restraint is associated with increased cortisol excretion in postmenopausal women. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences, 61(6), 628-633.
34 McLean, J. A., Barr, S. I., & Prior, J. C. (2001). Cognitive dietary restraint is associated with higher urinary cortisol excretion in healthy premenopausal women. The American journal of clinical nutrition, 73(1), 7-12.
35 Levine, J. A., Eberhardt, N. L., & Jensen, M. D. (1999). Role of nonexercise activity thermogenesis in resistance to fat gain in humans. Science, 283(5399), 212-214.
36 Tremblay, A., Royer, M. M., Chaput, J. P., & Doucet, E. (2013). Adaptive thermogenesis can make a difference in the ability of obese individuals to lose body weight. International journal of obesity, 37(6), 759.
37 Dulloo, A. G., Jacquet, J., Montani, J. P., & Schutz, Y. (2012). Adaptive thermogenesis in human body weight regulation: more of a concept than a measurable entity?. obesity reviews, 13, 105-121.
38 Rosenbaum, M., & Leibel, R. L. (2010). Adaptive thermogenesis in humans. International journal of obesity, 34(S1), S47.
39 Müller, M. J., & Bosy‐Westphal, A. (2013). Adaptive thermogenesis with weight loss in humans. Obesity, 21(2), 218-228.
40 Weyer, C., Vozarova, B., Ravussin, E., & Tataranni, P. A. (2001). Changes in energy metabolism in response to 48 h of overfeeding and fasting in Caucasians and Pima Indians. International journal of obesity, 25(5), 593.
41 Pontzer, H., Durazo-Arvizu, R., Dugas, L. R., Plange-Rhule, J., Bovet, P., Forrester, T. E., … & Luke, A. (2016). Constrained total energy expenditure and metabolic adaptation to physical activity in adult humans. Current Biology, 26(3), 410-417.
42 MacLean, P. S., Higgins, J. A., Johnson, G. C., Fleming-Elder, B. K., Donahoo, W. T., Melanson, E. L., & Hill, J. O. (2004). Enhanced metabolic efficiency contributes to weight regain after weight loss in obesity-prone rats. American Journal of Physiology-Regulatory, Integrative and Comparative Physiology.
43 Martin, C. K., Heilbronn, L. K., De Jonge, L., DeLany, J. P., Volaufova, J., Anton, S. D., … & Ravussin, E. (2007). Effect of calorie restriction on resting metabolic rate and spontaneous physical activity. Obesity, 15(12), 2964-2973.
44 Redman, L. M., Heilbronn, L. K., Martin, C. K., De Jonge, L., Williamson, D. A., Delany, J. P., & Ravussin, E. (2009). Metabolic and behavioral compensations in response to caloric restriction: implications for the maintenance of weight loss. PloS one, 4(2), e4377.
45 Rosenbaum, M., Hirsch, J., Gallagher, D. A., & Leibel, R. L. (2008). Long-term persistence of adaptive thermogenesis in subjects who have maintained a reduced body weight. The American journal of clinical nutrition, 88(4), 906-912.
46 Levine, J. A. (2002). Non-exercise activity thermogenesis (NEAT). Best Practice & Research Clinical Endocrinology & Metabolism, 16(4), 679-702.
47 Camps, S. G., Verhoef, S. P., & Westerterp, K. R. (2013). Weight loss, weight maintenance, and adaptive thermogenesis. The American of Clinical Nutrition, 97(5), 990-994.
48 Minster, R. L., Hawley, N. L., Su, C. T., Sun, G., Kershaw, E. E., Cheng, H., … & Urban, Z. (2016). A thrifty variant in CREBRF strongly influences body mass index in Samoans. Nature genetics, 48(9), 1049.
49 Weyer, C., Vozarova, B., Ravussin, E., & Tataranni, P. A. (2001). Changes in energy metabolism in response to 48 h of overfeeding and fasting in Caucasians and Pima Indians. International journal of obesity, 25(5), 593.
50 Reinhardt, M., Thearle, M. S., Ibrahim, M., Hohenadel, M. G., Bogardus, C., Krakoff, J., & Votruba, S. B. (2015). A human thrifty phenotype associated with less weight loss during caloric restriction. Diabetes, 64(8), 2859-2867.
51 Creasy, S. A., Rynders, C. A., Bergouignan, A., Kealey, E. H., & Bessesen, D. H. (2018). Free‐Living Responses in Energy Balance to Short‐Term Overfeeding in Adults Differing in Propensity for Obesity. Obesity, 26(4), 696-702.
52 Miles-Chan, J. L., Sarafian, D., Montani, J. P., Schutz, Y., & Dulloo, A. (2013). Heterogeneity in the energy cost of posture maintenance during standing relative to sitting: phenotyping according to magnitude and time-course. PloS one, 8(5), e65827.
53 Kotz, C. M., Teske, J. A., & Billington, C. J. (2008). Neuroregulation of nonexercise activity thermogenesis and obesity resistance. American Journal of Physiology-Regulatory, Integrative and Comparative Physiology, 294(3), R699-R710.
54 Schlögl, M., Piaggi, P., Pannacciuli, N., Bonfiglio, S. M., Krakoff, J., & Thearle, M. S. (2015). Energy expenditure responses to fasting and overfeeding identify phenotypes associated with weight change. Diabetes, 64(11), 3680-3689.
55 Wells, J. C. (2011). The thrifty phenotype: an adaptation in growth or metabolism?. American Journal of Human Biology, 23(1), 65-75.
56 Levine, J. A., Eberhardt, N. L., & Jensen, M. D. (1999). Role of nonexercise activity thermogenesis in resistance to fat gain in humans. Science, 283(5399), 212-214.
57 Reinhardt, M., Thearle, M. S., Ibrahim, M., Hohenadel, M. G., Bogardus, C., Krakoff, J., & Votruba, S. B. (2015). A human thrifty phenotype associated with less weight loss during caloric restriction. Diabetes, 64(8), 2859-2867.
58 Müller, M. J., Enderle, J., Pourhassan, M., Braun, W., Eggeling, B., Lagerpusch, M., … & Bosy-Westphal, A. (2015). Metabolic adaptation to caloric restriction and subsequent refeeding: the Minnesota Starvation Experiment revisited. The American journal of clinical nutrition, 102(4), 807-819.
59 Friedl, K. E., Moore, R. J., Hoyt, R. W., Marchitelli, L. J., Martinez-Lopez, L. E., & Askew, E. W. (2000). Endocrine markers of semistarvation in healthy lean men in a multistressor environment. Journal of Applied Physiology, 88(5), 1820-1830.
60 Hulmi, J. J., Isola, V., Suonpää, M., Järvinen, N. J., Kokkonen, M., Wennerström, A., … & Häkkinen, K. (2017). The effects of intensive weight reduction on body composition and serum hormones in female fitness competitors. Frontiers in physiology, 7, 689.
61 Astbury, N. M., Aveyard, P., Nickless, A., Hood, K., Corfield, K., Lowe, R., & Jebb, S. A. (2018). Doctor Referral of Overweight People to Low Energy total diet replacement Treatment (DROPLET): pragmatic randomised controlled trial. bmj, 362, k3760.
62 Huovinen, H. T., Hulmi, J. J., Isolehto, J., Kyröläinen, H., Puurtinen, R., Karila, T., … & Mero, A. A. (2015). Body composition and power performance improved after weight reduction in male athletes without hampering hormonal balance. The Journal of Strength & Conditioning Research, 29(1), 29-36.
63 Alajmi, N., Deighton, K., King, J. A., Reischak-Oliveira, A., Wasse, L. K., Jones, J., … & Stensel, D. J. (2016). Appetite and energy intake responses to acute energy deficits in females versus males. Medicine and science in sports and exercise, 48(3), 412.
64 Cameron, J. D., Goldfield, G. S., Riou, M. È., Finlayson, G. S., Blundell, J. E., & Doucet, É. (2016). Energy depletion by diet or aerobic exercise alone: impact of energy deficit modality on appetite parameters. The American journal of clinical nutrition, 103(4), 1008-1016.
65 Andro. (2014). High energy flux, a new determinant of successful weight Loss? eat more, train More, lose more? increased resting metabolic rate & satiety, decreased hunger while dieting! SuppVersity. Retrieved from http://suppversity.blogspot.com/2014/11/high-energy-flux-new-determinant-of.html
66 Hume, D. J., Yokum, S., & Stice, E. (2016). Low energy intake plus low energy expenditure (low energy flux), not energy surfeit, predicts future body fat gain. The American journal of clinical nutrition, 103(6), 1389-1396.
67 Kraemer, W. J., Volek, J. S., Clark, K. L., Gordon, S. E., Puhl, S. M., Koziris, L. P., … & HÄkkinen, K. (1999). Influence of exercise training on physiological and performance changes with weight loss in men. Medicine and science in sports and exercise, 31(9), 1320-1329.
68 Clark, J. E. (2015). Diet, exercise or diet with exercise: comparing the effectiveness of treatment options for weight-loss and changes in fitness for adults (18–65 years old) who are overfat, or obese; systematic review and meta-analysis. Journal of Diabetes & Metabolic Disorders, 14(1), 31.
69 Willis, L. H., Slentz, C. A., Bateman, L. A., Shields, A. T., Piner, L. W., Bales, C. W., … & Kraus, W. E. (2012). Effects of aerobic and/or resistance training on body mass and fat mass in overweight or obese adults. American Journal of Physiology-Heart and Circulatory Physiology.
70 Bryner, R. W., Ullrich, I. H., Sauers, J., Donley, D., Hornsby, G., Kolar, M., & Yeater, R. (1999). Effects of resistance vs. aerobic training combined with an 800 calorie liquid diet on lean body mass and resting metabolic rate. Journal of the American College of Nutrition, 18(2), 115-121.
71 Mekary, R. A., Grøntved, A., Despres, J. P., De Moura, L. P., Asgarzadeh, M., Willett, W. C., … & Hu, F. B. (2015). Weight training, aerobic physical activities, and long‐term waist circumference change in men. Obesity, 23(2), 461-467.
72 Schwingshackl, L., Dias, S., Strasser, B., & Hoffmann, G. (2013). Impact of different training modalities on anthropometric and metabolic characteristics in overweight/obese subjects: a systematic review and network meta-analysis. PloS one, 8(12), e82853.
73 Alberga, A. S., Prud’homme, D., Kenny, G. P., Goldfield, G. S., Hadjiyannakis, S., Gougeon, R., … & Ma, J. (2015). Effects of aerobic and resistance training on abdominal fat, apolipoproteins and high-sensitivity C-reactive protein in adolescents with obesity: the HEARTY randomized clinical trial. International journal of obesity, 39(10), 1494.
74 Geliebter, A., Maher, M. M., Gerace, L., Gutin, B., Heymsfield, S. B., & Hashim, S. A. (1997). Effects of strength or aerobic training on body composition, resting metabolic rate, and peak oxygen consumption in obese dieting subjects. The American journal of clinical nutrition, 66(3), 557-563.
75 Ho, S. S., Dhaliwal, S. S., Hills, A. P., & Pal, S. (2012). The effect of 12 weeks of aerobic, resistance or combination exercise training on cardiovascular risk factors in the overweight and obese in a randomized trial. BMC public health, 12(1), 704.
76 Sanal, E., Ardic, F., & Kirac, S. (2013). Effects of aerobic or combined aerobic resistance exercise on body composition in overweight and obese adults: gender differences. A randomized intervention study. Eur J Phys Rehabil Med, 49(1), 1-11.
77 Byrne, N. M., Sainsbury, A., King, N. A., Hills, A. P., & Wood, R. E. (2018). Intermittent energy restriction improves weight loss efficiency in obese men: the MATADOR study. International journal of obesity, 42(2), 129.
78 Davoodi, S. H., Ajami, M., Ayatollahi, S. A., Dowlatshahi, K., Javedan, G., & Pazoki-Toroudi, H. R. (2014). Calorie shifting diet versus calorie restriction diet: a comparative clinical trial study. International journal of preventive medicine, 5(4), 447.
79 Davoodi, S. H., Hajimiresmaiel, S. J., Ajami, M., Mohseni-Bandpei, A., Ayatollahi, S. A., Dowlatshahi, K., … & Pazoki-Toroudi, H. (2014). Caffeine treatment prevented from weight regain after calorie shifting diet induced weight loss. Iranian journal of pharmaceutical research: IJPR, 13(2), 707.
80 Seimon, R. V., Shi, Y. C., Slack, K., Lee, K., Fernando, H. A., Nguyen, A. D., … & Herzog, H. (2016). Intermittent moderate energy restriction improves weight loss efficiency in diet-induced obese
81 Dirlewanger, M., Di Vetta, V., Guenat, E., Battilana, P., Seematter, G., Schneiter, P., … & Tappy, L. (2000). Effects of short-term carbohydrate or fat overfeeding on energy expenditure and plasma leptin concentrations in healthy female subjects. International journal of obesity, 24(11), 1413.
82 Romon, M., Lebel, P., Velly, C., Marecaux, N., Fruchart, J. C., & Dallongeville, J. (1999). Leptin response to carbohydrate or fat meal and association with subsequent satiety and energy intake. American Journal of Physiology-Endocrinology And Metabolism, 277(5), E855-E861.